26 February 2026
Shri Dinesh Gundu Rao
Honorable Minister of Health and Family Welfare
Government of Karnataka
Subject: Recommendations for a Comprehensive Right to Health Act for Karnataka
Respected Sir,
We commend the Government of Karnataka for its progressive step in drafting The Karnataka Right to Health and Emergency Medical Service Bill, 2025. However, the draft requires extensive improvement to truly realize a rights-based health framework. The entitlements it defines are very vague and the accountability provisions are very weak. We urge the following modifications.
1. Integration of Social Determinants and Public Health
- Enact a Public Health Act: Karnataka lacks a legislative framework for the prevention of communicable diseases and outbreak notification. We urge the government to integrate Public Health Act provisions – similar to 2009 Gujarat or separate one like Tamil Nadu – to address social determinants like water, nutrition, and sanitation.
2. Operationalizing the Right to Health Care
- Universal Health System: The Act should bring all public and private providers under a unified Universal Health System to ensure seamless, dignity-based care.
- Free medicines, diagnostics and treatment in public facilities with complete removal of user fees: Access to health must not depend on the ability to pay. The Act should guarantee free treatment, diagnostics, and quality medicines at all public facilities.
- Community Participation and Redressal: Residents must be empowered as active participants in planning and design, supported by robust grievance redressal mechanisms.
- Justiciability: To be a true “Right,” denials of care must be made justiciable in court.
3. Effective Regulation of the Private Sector
- Beyond Licensing: The current draft is largely silent on private sector regulation. While the KPME Act exists, it is primarily for licensing.
- Autonomous Regulatory Body: Following the Vision Committee of Karnataka report, we recommend establishing an autonomous regulatory body to oversee costs, quality, and the implementation of such measures as standard treatment guidelines.
We believe the 2009 National Right to Health Bill can serve as a foundational blueprint that Karnataka can adapt to create an exemplary legislative template for the nation.
We attach a summary framework for a Right to Health Act, drawn from various bills across the country. We urge the Ministry to hold inclusive public consultations and revise the draft thoroughly before tabling it in the Assembly. We would be happy to engage with the health department in a constructive manner and support the Ministry in refining this landmark endeavour.
Yours sincerely,
For Sarvatrika Arogya Andolana Karnataka
CC:
Ms. Uma Mahadevan, Additional Chief Secretary, Government of Karnataka.
Mr. Harsh Gupta, Principal Secretary, Ministry of Health and Family Welfare, Government of Karnataka.
Summary of comments
We commend the state of Karnataka for making the first move towards a Right to Health Act through the drafting of the bill. It reflects lessons from the Rajasthan experience and introduces emergency care provisions in the bill. It has a provision of Director of Emergency Medical Services (Chapter III) which is very unique and goes a long way in ensuring access to medical emergency services including ambulance services and facility based care. However, the said act is not a comprehensive Right to Health Act as outlined in the following sections, nor does it contain the minimum features of an effective Right to Health Act.The entitlements it defines are vague and the accountability provisions are very weak.
Karnataka requires a public health act to address the social determinants of health. It can follow the Gujarat draft bill of 2009 which has tried to integrate the public health act provisions into the Right to Health bill or it can choose to have a separate one as in Tamil Nadu. The act is largely silent on the various provisions necessary to operationalise right to health care including various treatments, preventive and promotive services and community participation. Even the basic entitlement to free healthcare in public institutions is not clearly spelt out. The 2009 National Right to Health Bill serves as a foundational blueprint, offering a ready-made legislative template for the state right to health act.
The current bill is silent on regulation of the private sector. Even at the national level, none of the current state and national level drafts provide for effective regulation of the private sector. All the drafts rely heavily upon the different clinical establishments Act present in different states. The Karnataka government has the advantage of drawing upon the Vision Committee report to bring in mechanisms for regulation of the private sector.
We consider it essential that this draft Bill should be placed in the public domain, submitted to inclusive consultations, and extensively revised before being tabled in the Assembly.
–——————–
Background and Rationale
India is a signatory to many International Human Rights Agreements most of which have underlined that Health is a Human Right. India has signed the UN declaration of Human Rights which states that health as a human right is a basic tenet (article 25). In 1965, India also was a signatory to the International Covenant on economic, social and cultural rights (ICESCR) which reiterated that health is a human right (Article 12). India signed the Alma Ata Declaration in 1978 which declared Health as a Human Right as one of the fundamental principles. In the Constitution of India, Article 21 which deals with Right to Life (under which right to health is encompassed by the Supreme Court of India) as a fundamental right. Since health management falls under the jurisdiction of individual states, the Constitution places the duty to pass ‘right to health’ acts within the Directive Principles, making them guidelines for governance rather than immediate legal requirements. (Article 38, 39, 42, 43 and 47).
Given this background and commitment to Right to Health by the framers of the Constitution, it is important that the Government of Karnataka takes the necessary steps to enact a Right to Health Act. Karnataka has reached a very commendable position of the highest per capita income in the country. Given this, it behoves the Government of Karnataka to come up with a Right to Health Act in the state.
Karnataka’s health indicators, though better than India level indicators, are the worst among the other southern Indian states. The Maternal Mortality ratio (MMR) is at 69, even though it has improved from 228 in 2001-2003, it is still nowhere near Kerala’s level of 19. Similarly, when it comes to Infant mortality rate (IMR), Karnataka has an IMR of 14 as compared to Kerala at 5. In Karnataka, 65.5 percent of children between the ages 6 months to 5 years are anaemic so are women who comprise 48 percent. Of course, the averages mask the inequalities within the state with districts like Raichur and Bidar performing much worse. At the same time, Karnataka’s health system is characterised by what is called as ‘Mixed Health Systems Syndrome’ – a dominant poorly regulated private sector and a weak public health sector.
It is universally acknowledged that health of the population is achieved through actions outside of the health sector – nutrition, water, sanitation, housing and such others. These are called the social determinants of health (SDH). The spirit of Alma Ata declaration of Health for All and Right to Health were based on Rights to the social and economic determinants of health. Thus, any Right to Health Act has to comprise 3 components:
- Right to the Social Determinants of health – Right to water, Right to food etc.
- Right to Health Care
- Regulation of the private sector for costs and quality
In addition to enacting rights for individual sectors like food, employment, water, there is also what is called a Public Health Act. Many states like Tamil Nadu have for a long-standing Public Health Act in place. Karnataka lacks a Public Health Act to address prevention of spread of communicable diseases, notification of outbreak of diseases and such other provisions. Thus, Karnataka has to enact a Public Health Act. There are many models in the country which can be emulated to bring about such an Act.
Right to Health Care Act
A Right to Health Care Act would govern the functioning of health systems. Such an act is a means through which residents of the state are entitled to free, quality, dignified care with adequate grievance redressal mechanisms. Right to Health Care Act can comprise of 3 major dimensions:
a) Health care services (curative)
b) Preventive and promotive care
c) Palliative and rehabilitative care.
The following should be incorporated in the Right to Health Care Act
- Bring all public, private for profit and private not-for-profit under a Universal Health system.
- Ensure free and quality medicines in all the public facilities.
- Ensure free diagnostic facilities in the public facilities.
- Ensure free treatment in public facilities with no user fees. User fees are the most inequitable form of financing health and run counter to the entitlements that are foundational in a Right to Health Care Act if people’s access to health care is dependent on their ability to pay.
- Staffing issues to be addressed urgently. Adequate staff and infrastructure to be ensured in accordance with the Indian Public Health Standards (IPHS) 2022.
- Ensure comprehensive care is available in public facilities. Comprehensive care shall have the right to – emergency services; preventive and promotive services; women’s health, maternal and child services; primary, secondary and tertiary care services; rehabilitation services; geriatric services and so on. In principle, all of these must be available within the gamut of services unless there’s epidemiological evidence to the contrary. This also means seamless integration of care from the primary to tertiary levels with assisted referrals also to private sector as a last resort, in case the particular treatment is not available at that facility.
- Ensure Patients’ rights as defined by the National Human Rights Commission and included in the Clinical Establishments Act 2010.
- Ensure non-discrimination on the basis of caste, class, religion, gender, disabilities and ethnicities and provide dignity of care with staff sensitised for respectful care.
- Ensure community participation at all levels of the care for communities to meaningfully participate not just as a beneficiary of services but as active empowered residents planning, designing and overseeing of the care.
- Include grievance redressal mechanisms for timely redressal of grievances at the facility level with the provision of ombudspersons. Denials of the rights must also be justiciable in the courts of the land with provisions for escalation to higher courts. With a universal health system, community participation and grievance redressal can function even in non-state actors and hold them accountable as well.
- Build the capacities of the staff in accordance with the Right to Health Act.
- Home based primary care must be available for those with disability and those requiring long-term, high frequency care
- Emergency medical transportation including emergency access roads, especially in tribal areas
- All rights should apply for migrant workers too. Special provisions for homeless, migrants, and informal sector workers.
- Put in place strong Anti-Corruption Measures.
- Special training for providing affirmative care to gender and sexually diverse individuals
Regulating the Private Sector
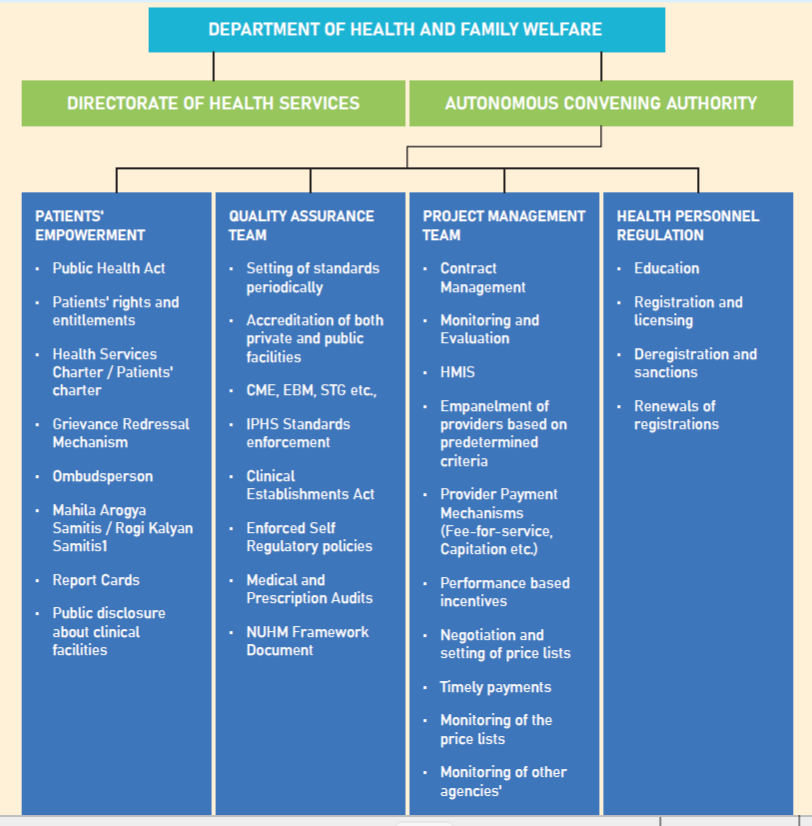
India has one of the most unregulated private sectors in the world in which the care is largely irrational, unethical and expensive. As part of the Right to Health Act, the government of Karnataka must bring in largescale regulation of costs, quality and rationality into the private sector. There is a misconception that the Karnataka Private Medical Establishments Act (KPME) is there to regulate the private sector. KPME is only a licensing and registration act – necessary but insufficient. Regulatory mechanisms must ensure evidence-based medicines, standard treatment guidelines, patients’ rights, and regulation of costs . Chapter 22 of the Vision Committee of Karnataka report suggested a range of measures to regulate the private sector starting with an autonomous regulatory body under the Ministry of Health and Family Welfare with adequate staff and infrastructure. The government must use its monopsony power under a universal health system to regulate the private sector. The following schematic was proposed as part of the chapter in the Vision committee. As part of the Right to Health Act, the government should progressively implement these mechanisms to regulate the private sector in these areas.